
2022-2023 Influenza Season Looks to Be Severe

Outpatient treatment is primarily based on patient-specific factors, whereas oseltamivir remains the therapy of choice for inpatient settings.
Despite a very mild influenza season the past 2 years, the 2022-2023 influenza season has the potential to cause significant stress to an already overburdened US health care system. For 2021-2022, the flu positivity rate was historically low at 4.5%. This was largely because of increased COVID-19 restrictions and flu testing that may have lowered the positivity rate.1 However, in many parts of the country, a surge late in the last flu season is expected to continue into next season.
Low antibody levels related to low exposure, poor exposure, and relaxed COVID-19 restrictions all played parts in the latest flu surge. Initial prelimi-nary reports released in October 2021 showed that this year’s flu vaccines were not significantly effective at reducing illness due to influenza A (H3N2), with a 16% overall vaccine effectiveness rate.2 However, a June 2022 report from the CDC’s Advisory Committee on Immuniza-tion Practices (ACIP) showed effectiveness rates of 34% (95% CI, 19%-46%), which is in line with what is typically observed.3
The CDC has selected new flu vaccines that were available in August 2022, with a major change in the selection of the H3N2 and influenza B components.4 Additionally, the FDA approved a change in the recom mended age for the Flucelvax Quadrivalent between ages 6 months and 4 years. The ACIP also recommends that adults aged at least 65 years receive 1 of the following adjuvanted or high-dose vaccines4:
- Quadrivalent adjuvanted inactivated influenza vaccine
- Quadrivalent high-dose inactivatedinfluenza vaccine
- Quadrivalent recombinantinfluenza vaccine
Therapeutic Management of Influenza
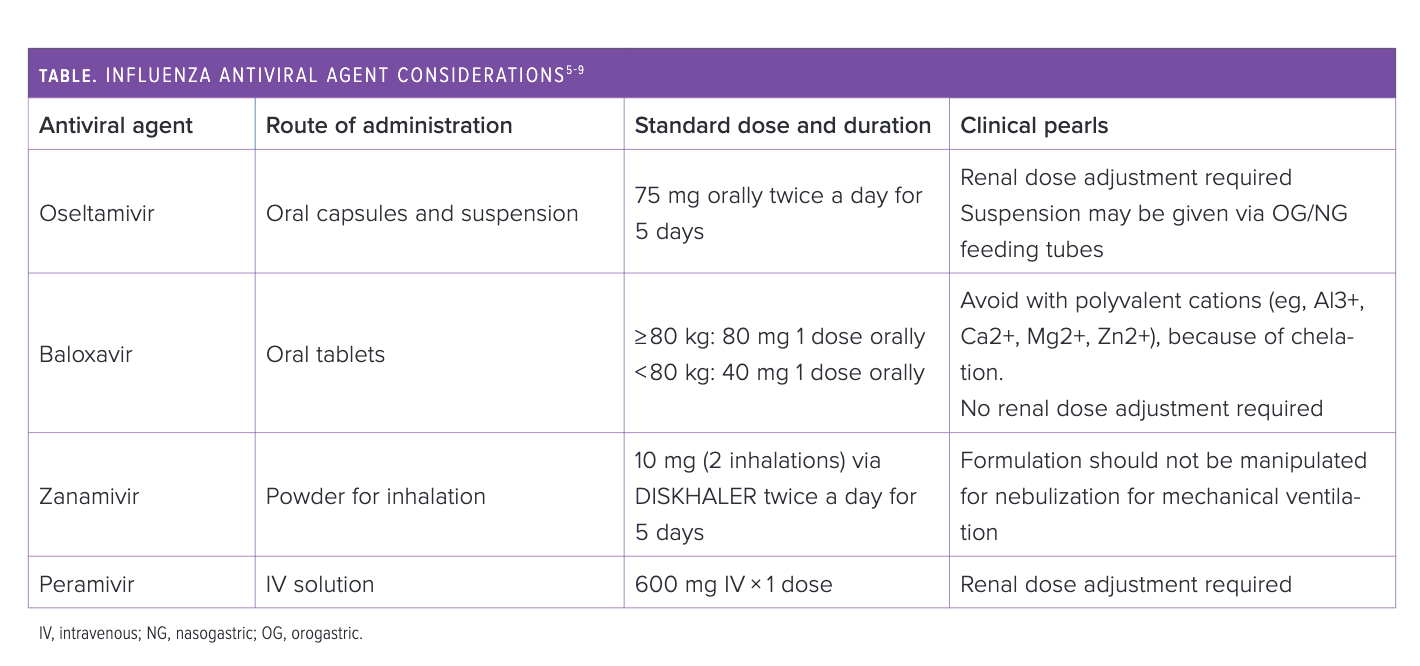
Antiviral treatments of influenza A and B are listed in the Table.5-9 Oseltamivir, peramivir, and zanamivir are viral neur-aminidase inhibitors, which prevent the release of viral particles from the plasma membrane of infected human cells.5-8 Baloxavir introduced a novel mechanism of action through inhibition of viral repli-cation by inhibiting the polymerase acidic protein within the viral RNA polymerase.9 Antiviral treatment should be initiated as soon as possible, with the greatest benefit observed when started within 48 hours of symptom onset.9-10 Antiviral-specific considerations are outlined in the Table.5-9


Outpatient Influenza Management
The primary benefit of influenza treatment in the outpatient setting is a reduction in fever and symptoms by 1 to 2 days.9-11 In patients with risk factors for influenza complications, there is an added benefit of lowering the likelihood of hospitalization.9 The CDC recommends equally all the aforementioned antivirals for outpatient antiviral therapy.10 The results of recent literature suggest baloxavir may be linked to additional benefits, such as rates of influenza-related complications and reduced health care–related costs.12,13 Furthermore, baloxavir offers a treatment option when there is concern for neuraminidase inhibitor resistance. However, this is balanced with the risk of baloxavir treatment-emergent resistance.11 The treatment duration with oseltamivir and zanamivir is 5 days, whereas baloxavir and peramivir require only a single dose.7-9
Inpatient Influenza Management
Oseltamivir remains the preferred agent for hospitalized patients, as data are limited for other treatment options. The results of observational studies have shown that oseltamivir may reduce the duration of hospitalization and mortality. Although the most significant benefit is seen when antiviral treatment is started within 48 hours of symptom onset, oseltamivir still has benefit when started within 4 to 5 days, and possibly up to 7 days, from symptom onset. Treatment duration is 5 days, although the duration may be extended to 10 days or longer in patients who are immunocompromised or those with severe lower respiratory tract disease.9 In patients with poor oral access or malabsorption, peramivir is a treatment option10; however, peramivir was studied in hospitalized patients in a randomized trial and did not show a significant clinical benefit.14 But the CDC suggests peramivir should still be considered for hospitalized patients who are unable to take oral medications.10
Conclusion
The upcoming influenza season may be more severe because of low circulating anti-body levels and relaxed mask restrictions. Outpatient treatment is primarily based on patient-specific factors, whereas oseltamivir remains the treatment of choice forinpatient settings.
References
1. Weekly U.S. influenza surveillance report. CDC. Accessed August 17, 2022. https://www.cdc.gov/flu/weekly/index.htm
2. Chung JR, Kim SS, Kondor RJ, et al. Interim estimates of 2021-22 seasonal influenza vaccine effectiveness - United States, February 2022. MMWR Morb Mortal Wkly Rep. 2022;71(10):365-370. doi:10.15585/mmwr.mm7110a1
3. Preliminary estimates of 2021–22 seasonal influenza vaccine effectiveness. CDC. June 22, 2022. Accessed August 19, 2022. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2022-06-22-23/02-influenza-Chung-508.pdf
4. Grohskopf L. Influenza Work Group: summary and proposed recommendations for the 2022-23 influenza season. CDC. June 22, 2022. Accessed August 19, 2022. https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2022-06-22-23/04-influenza-grohskopf-508.pdf
5. Tamiflu. Prescribing information. Genentech; 2012. Accessed August 19, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/021087s062lbl.pdf
6. Relenza. Prescribing information. GlaxoSmithKline; 2010. Accessed August 19, 2022.
https://www.accessdata.fda.gov/drugsatfda_docs/label/2010/021036s025lbl.pdf
7. Rapivab. Prescribing information. BioCryst Pharmaceuticals Inc; 2014. Accessed August 19, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2014/206426lbl.pdf
8. Xofluza. Genentech; 2018. Accessed August 19, 2022. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/210854s000lbl.pdf
9. Uyeki TM, Bernstein HH, Bradley JS, et al. Clinical practice guidelines by the Infectious Diseases Society of America: 2018 update on diagnosis, treatment, chemoprophylaxis, and institutional outbreak management of seasonal influenzaa. Clin Infect Dis. 2019;68(6):e1-e47. doi:10.1093/cid/ciy866
10. Influenza antiviral medications: summary for clinicians. CDC. Updated August 16, 2022. Accessed July 2, 2022. https://www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm
11. Hayden FG, Sugaya N, Hirotsu N, et al. Baloxavir marboxil for uncomplicated influenza in adults and adolescents. N Engl J Med. 2018;379(10):913-923. doi:10.1056/NEJMoa1716197
12. Neuberger E, Wallick C, Chawla D, Castro RC. Baloxavir vs oseltamivir: reduced utilization and costs in influenza. Am J Manag Care. 2022;28(3):e88-e95. doi:10.37765/ajmc.2022.88786
13. Liu JW, Lin SH, Wang LC, Chiu HY, Lee JA. Comparison of antiviral agents for seasonal influenza outcomes in healthy adults and children: a systematic review and network meta-analysis. JAMA Netw Open. 2021;4(8):e2119151. doi:10.1001/jamanetworkopen.2021.19151
14. de Jong MD, Ison MG, Monto AS, et al. Evaluation of intravenous peramivir for treatment of influenza in hospitalized patients. Clin Infect Dis. 2014;59(12):e172-e185. doi:10.1093/cid/ciu632
About the Authors
John P. Bomkamp, PharmD, BCPS-AQ ID, is an infectious diseases clinical pharmacist at Indiana University Health in Indianapolis.
Amer El-Ghali, PharmD is an infectious diseases pharmacokinetic/pharmacodynamic and health outcomes research fellow at the Anti-Infective Research Laboratory at Wayne State University in Detroit, Michigan.


























